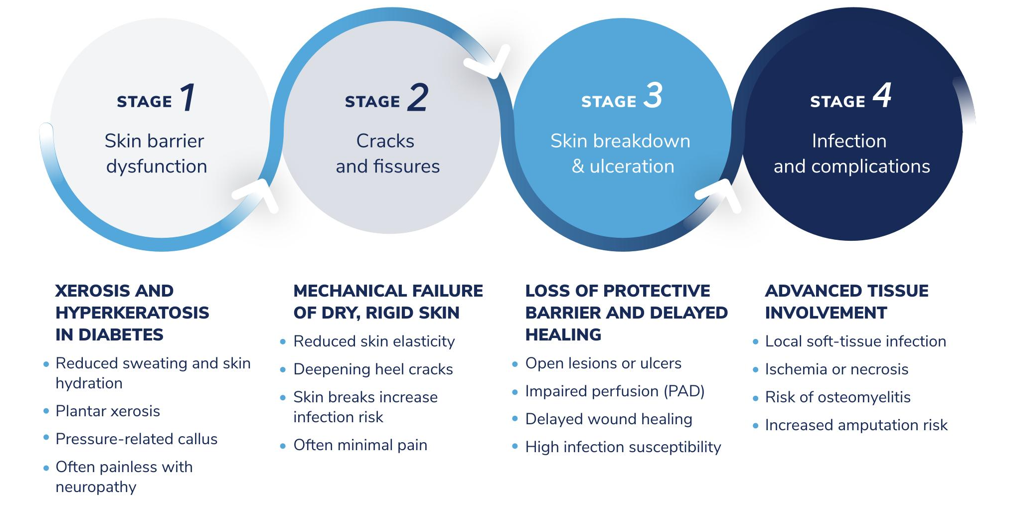
Why are feet at risk in diabetes?
Identifying diabetic foot risk in pharmacy practice
In people with diabetes, pharmacists frequently encounter dry skin, hard skin build-up, cracked heels, fissures, calluses, corns, nail disorders, as well as minor cuts, blisters, and fungal infections. Importantly, the absence of pain does not indicate low risk, particularly in individuals with established or suspected neuropathy. Reduced or altered sensation may not be apparent without assessment using simple clinical tools, such as a neurotip, which many pharmacies may have access to; however, appropriate training in their use is essential 5. Where neuropathy is suspected, referral to a podiatrist for formal sensory testing as part of a comprehensive foot examination is recommended. Any break in the skin should be considered potentially significant 2, 6, 7.
When a person with diabetes presents with a foot concern, pharmacists should begin by asking exploratory questions to better understand the context. These may include how long the issue has been present, whether there have been previous foot problems or ulceration, the presence or absence of pain, and the duration of diabetes. Establishing this background helps identify potential risk factors and urgency.
Where appropriate, visual inspection should then check for broken skin, redness, swelling, discharge, or color changes. Poorly fitting footwear and difficulty with self-care further increase risk. Any abnormal finding should prompt referral 6-8.
Supporting daily foot care and maintenance
Preventive management of foot problems in people with diabetes begins with patient education. Community pharmacists are often the first point of contact for patients raising foot concerns, placing them in a key position to reinforce preventive behaviors and early risk awareness.
International guidelines recommend that people with diabetes adopt consistent daily foot care habits. These include daily foot inspection, careful washing and thorough drying, and the regular use of moisturizers on dry skin to help prevent cracking, while avoiding application between the toes 6, 7.
Advice on safe nail care, appropriate footwear, and avoiding barefoot walking is also essential. Importantly, patients should know where to seek advice promptly if they notice any skin break, color change, swelling, or other new concerns, even in the absence of pain 6, 7, 9.
The role of insoles and topical care in diabetic foot prevention
Foot abnormalities in people with diabetes may arise due to structural changes associated with neuropathy, the ageing process, and pre-existing foot shape. These factors can create areas of increased plantar pressure and friction, which, over time, may contribute to skin breakdown.
International guidance recognizes that simple pressure-relieving insoles may be appropriate for individuals at low risk of ulceration. By helping to redistribute pressure, improve shock absorption, and enhance overall comfort and protection, insoles can support a broader preventive strategy aimed at maintaining skin integrity 6, 7.
At the same time, regular use of moisturizers supports skin hydration and helps maintain barrier function. Formulations containing urea may be particularly beneficial in reducing dryness and hard skin build-up. Maintaining skin suppleness and flexibility is important in helping to lower the risk of cracking and fissure formation.
Mechanical support and appropriate topical care therefore work together as part of routine preventive management in people with diabetes 9-11.
Product selection and referral considerations
In people with diabetes considered low risk, pharmacists can support preventive care and advise on appropriate footcare products. However, ulcers, open wounds, or signs of infection require medical assessment and referral.
When recommending OTC treatments, ingredient choice matters. Products containing salicylic acid (including some corn plasters and corn-removal treatments) may not be appropriate for use on diabetic feet due to the action of the ingredient and the increased risk of skin damage, particularly where sensation is reduced.
To support appropriate product choice, Dr. Scholl’s products include a diabetes recommendation to help guide safe use for both patients and pharmacists 6, 8.
Red flags requiring urgent referral
Pharmacists should advise urgent medical assessment if any of the following are identified during a consultation:
- Ulcers or any open wounds
- Signs of infection: increasing redness, warmth, swelling, pain/tenderness, or discharge
- Blackened or necrotic skin
- New foot deformity
- Sudden or unexplained changes in sensation
These features indicate a high risk of serious complications and require prompt specialist evaluation
- Armstrong, D.G., A.J.M. Boulton, and S.A. Bus, Diabetic Foot Ulcers and Their Recurrence. N Engl J Med, 2017. 376(24): p. 2367-2375.
- van Netten, J.J., et al., Definitions and criteria for diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab Res Rev, 2024. 40(3): p. e3654.
- Pop-Busui, R., et al., Diabetic Neuropathy: A Position Statement by the American Diabetes Association. Diabetes Care, 2017. 40(1): p. 136-154.
- Srinivas-Shankar, U., A. Kimyaghalam, and R. Bergman, Diabetic Foot Ulceration and Complications, in StatPearls. 2025: Treasure Island (FL) relationships with ineligible companies. Disclosure: Ali Kimyaghalam declares no relevant financial relationships with ineligible companies. Disclosure: Rachel Bergman declares no relevant financial relationships with ineligible companies.
- Matalqah, L.M., A. Yehya, and K.M. Radaideh, Pharmacist-lead screening for diabetic peripheral neuropathy using Michigan Neuropathy Screening Instrument (MNSI). Int J Neurosci, 2024. 134(8): p. 882-888.
- Schaper, N.C., et al., Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab Res Rev, 2024. 40(3): p. e3657.
- Senneville, E., et al., IWGDF/IDSA guidelines on the diagnosis and treatment of diabetes-related foot infections (IWGDF/IDSA 2023). Diabetes Metab Res Rev, 2024. 40(3): p. e3687.
- in 2019 surveillance of diabetes (NICE guidelines NG17, NG18, NG19 and NG28). 2019: London.
- Bus, S.A., et al., Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2023 update). Diabetes Metab Res Rev, 2024. 40(3): p. e3651.
- Ren, Y., et al., Advancements in diabetic foot insoles: a comprehensive review of design, manufacturing, and performance evaluation. Front Bioeng Biotechnol, 2024. 12: p. 1394758.
- Piquero-Casals, J., et al., Urea in Dermatology: A Review of its Emollient, Moisturizing, Keratolytic, Skin Barrier Enhancing and Antimicrobial Properties. Dermatol Ther (Heidelb), 2021. 11(6): p. 1905-1915.